Our bodies like to remind us that we aren’t as young as we used to be. The good news is that our digestive systems aren’t affected by aging as much as the other parts of us [1]. The bad news is that we can’t abuse our stomachs like we used to if we want to maintain the pleasure of eating. Does this mean that we have developed food intolerance? Not necessarily. To see why, let’s first look at the normal gastrointestinal signs of getting older, along with some age-related complications.
Age-related changes in digestion
Age brings with it certain changes in digestive function that some healthy people may notice more than others, including [2]:
Decreased lactase production. Older adults are more likely to be lactose intolerant and experience bloating, gas, or diarrhea after eating dairy products.
Decreased elasticity and slower emptying of the stomach. Some people cannot eat as much as they used to in one sitting without feeling fullness or bloating.
Overgrowth of certain bacteria in the small intestine. Our gut bacteria is mostly confined to the large intestine, and this is normal (although some bacteria are more desirable than others). As we age, the chance of bacterial overgrowth in the small intestine increases, producing pain, bloating, and weight loss.
Slowing or weakening of contractions in the large intestine. Constipation is more likely as we age.
If any of these points sound familiar, speak with your doctor to make sure that your symptoms are simply age-related and not part of a more serious problem. Be sure to discuss any signs of small intestinal bacterial overgrowth, because even though you can find plenty of Internet advice about “healing your gut” on your own, this condition may need medical treatment.
Other gastrointestinal symptoms are not caused by aging per se, but by things that go along with age [3], such as:
Medications. These can increase or decrease the time it takes for food to pass through us, resulting in either constipation or loose stools.
Age-related illnesses. Certain illnesses can also affect the proper functioning of the digestive system.
Obesity. Obesity makes heartburn more likely.
Continuing bad eating habits. Late-night fast food or too much coffee can cause heartburn and affect intestinal transit time.
In these cases, something as simple as a change in medication could provide much relief. As I said before, talk with your doctor about your concerns.
Relationship with food intolerance
If someone experiences a bad reaction after eating a certain food, it’s easy to understand why they might conclude that they have food intolerance – after all, it’s almost impossible to escape the association between food and digestion. But true food intolerance is a hypersensitivity reaction to food (emphasis on hyper-sensitivity) that most people will not encounter.
Continuing with our original question, are any age-related symptoms actually food intolerance? Well, there are three types of food intolerance [4,5]:
Enzymatic food intolerance – when the body does not make enough enzymes to digest or properly use a nutrient, as in lactose intolerance or phenylketonuria.
Toxic reactions – mainly histamine toxicity from spoiling fish (scombroid poisoning)
According to this classification, lactose intolerance is a type of food intolerance, but the other age-related digestive symptoms are not. This is an important distinction to make with regards to how we think about (and act on) our current state of health – in other words, do we continue to view ourselves as “normal” for our age, or do we start to feel like we have a “problem”?
What does this mean?
When food-related symptoms occur more frequently with age, this does not necessary mean that we have developed a medical problem – food intolerance – that needs to be treated by completely avoiding certain foods. It might just mean the we need to change our eating habits, like when we eat, how much we eat, and how much we can expect to indulge. For example, an adult with lactose intolerance may still be able to eat small amounts of dairy products (like yogurt) throughout the day, but they shouldn’t expect to go out after a soccer game and eat an ice cream sundae on an empty stomach like the rest of the kids. That said, if you are experiencing any of the symptoms mentioned in this article, see your doctor before attributing them to age.
3. Karen E. Hall, Wiley JW. Age-Associated Changes in Gastrointestinal Function. In: Hazzard W, et al. editors. Principles of Geriatric Medicine and Gerontology. 4th ed. New York: Mcgraw-Hill; 1998. p. 835–42.
4. Boyce JA, Assa’ad A, Burks AW, Jones SM, Sampson HA, Wood RA, et al. Guidelines for the Diagnosis and Management of Food Allergy in the United States: Summary of the NIAID-Sponsored Expert Panel Report. J Allergy Clin Immunol. 2010 Dec;126(6):1105–18. http://dx.doi.org/10.1016/j.jaci.2010.10.008
Food intolerance blood tests measure a person’s levels of IgG antibodies to a wide variety of foods, but IgG antibodies do not have any proven link to illness. At best, these blood tests are a waste of money; at worst, they can lead to poor or even dangerous health decisions.
Despite their inherent ineffectiveness, IgG food intolerance tests have spread to the pharmacy and the doctor’s office, making it hard for the average patient to know where to turn for reliable information. To protect the public, professional medical associations in many countries asked the best minds in immunology to prepare position statements warning against these tests. Let’s take a look at some of the main points from these warnings in plain English.
From the Australasian Society of Clinical Immunology and Allergy [1]:
“IgG antibodies to food are commonly detectable in healthy adult patients and children, independent of the presence or absence of food-related symptoms. There is no credible evidence that measuring IgG antibodies is useful for diagnosing food allergy or intolerance, nor that IgG antibodies cause symptoms. In fact, IgG antibodies reflect exposure to allergen but not the presence of disease.”(full text)
What it means
The most important thing to remember is that everyone produces IgG antibodies to food. The concentration of IgG antibodies in your blood depends on your genes, your diet, and maybe even on how you were fed as an infant [2]. There is simply no ‘correct’ IgG level. This means that a healthy person could get the same diet recommendations from an IgG blood test as a person with symptoms.
Looking at the entire body of available evidence, there is no correlation, let alone a causal link, between IgG antibodies and symptoms. In fact, using IgG test results to identify problem foods is no more successful than flipping a coin.
From the European Academy of Allergy and Clinical Immunology [2]:
“Food-specific IgG4 does not indicate (imminent) food allergy or intolerance, but rather a physiological response of the immune system after exposition to food components. Therefore, testing of IgG4 to foods is considered as irrelevant for the laboratory work-up of food allergy or intolerance and should not be performed in case of food-related complaints.”(full text)
What it means
You might think that not being allergic to a food – in other words, being “tolerant” to that food – means that your immune system ignores it. Sometimes that happens, but tolerance is often an active process. Regulatory T cells keep the immune system from reacting to potential food allergens, and it is these cells that call in the IgG antibodies by secreting an anti-inflammatory messenger chemical known as IL-10. IgG antibodies are not the sign or cause of anything bad, but rather a sign that a person has eaten and has tolerated a certain food. IgG antibodies have nothing to do with food intolerance.
From the Canadian Society of Allergy and Clinical Immunology [3]:
“The test is also being marketed to concerned parents, and may lead to exclusion diets which carry risks of poor growth and malnutrition for their children: for example, the elimination of dairy products, wheat, eggs, and/or other foods found in healthy balanced diets.”(full text)
What it means
IgG blood tests often identify between 5 and 20 suspect foods, so the risk of nutritional deficiencies in children is real if too many foods are eliminated without proper medical support. The bigger issue is whether these tests are actually related to the conditions they are purported to treat, namely ADHD and autism spectrum disorder (ASD); let’s take a look at that.
ADHD. Some artificial colors have been shown to affect behavior in children with ADHD, but this reaction does not involve the immune system, so IgG blood tests are irrelevant for identifying which children might be affected. Other foods have also been shown to aggravate ADHD, but IgG levels could not accurately predict which foods. [4]
Autism spectrum disorder. Since IgG blood tests do not really detect adverse reactions to foods, it is unlikely that these tests would apply specifically to autism. While there is speculation that a ‘leaky gut’ increases the likelihood that IgG antibodies to wheat and milk proteins will be found in the blood of children with ASD, a much-touted paper on the topic actually showed that IgG levels did not correlate with intestinal permeability [5].
This doesn’t mean, though, that someone with autism couldn’t also suffer from food intolerance independent of IgG test results. For parents thinking about dietary interventions for autism, it might be helpful to consider the opinion of registered dietitian Zoe Connor, chair of the Dietitians in Autism group within the British Dietetic Association [6]:
“…[A]lthough there is insufficient evidence to recommend the use of any diet as a treatment for ASD, dietitians and other health professionals should provide support when an individual or their parents choose to try dietary changes. There are too many reports of children with ASD improving in behaviour and/or bowel habits after eliminating some foods for them to be discounted. However, the mechanism for this (until proven otherwise) is likely to be the same as for any general food intolerance, rather than any specific disorder that is particular to ASD, and so each case should be considered individually. For example, bowel problems such as diarrhoea or constipation can sometimes be caused by food intolerances, so individuals suffering from these might benefit from trying different food exclusions (medical causes should first be investigated by a doctor).” (p. 66)
From the American Academy of Allergy Asthma and Immunology [7]:
“Additionally, and perhaps of greater potential concern, a person with a true immunoglobulin E (IgE)-mediated food allergy, who is at significant risk for life-threatening anaphylaxis, may very well not have elevated levels of specific IgG to their particular allergen, and may be inappropriately advised to reintroduce this potentially deadly item into their diet.”(full text)
What it means
In true food allergies, IgE antibodies bind with allergen proteins to cause chemicals, like histamine, to be released in the body and trigger symptoms. IgG antibodies are not interchangable with IgE antibodies, and IgG blood tests do not detect food allergies.
We most often think of food allergies as beginning in childhood, but adults can also develop allergies at any time. Perhaps an old allergy returns, perhaps a mild allergy was there in the background all along, or perhaps the allergy is completely new. New allergies to pollen can also bring on food-related symptoms in the form of oral allergy syndrome. Adult food allergies must be taken seriously, because the risk for severe reactions becomes greater the later they develop [8].
Approaching food sensitivities the right way
The EAACI position statement [1] mentions another vulnerable market for food intolerance blood tests – people who see their doctor for a suspected food sensitivity that turns out not to be an allergy but cannot be explained. The doctor dismisses their symptoms, but not their suspicions of food. Feeling let down, they go outside the medical community for care or advice – which is understandable, but never the wise thing to do.
In a case like this, the safest thing is to get a doctor’s referral to see a registered dietitian and discuss doing a diet investigation. Alternative medicine may use rhetoric about ‘hidden food intolerances,’ but a knowledgable dietitian can use your personal history and diet log to guide you through the elimination diet and food challenges that check for food intolerance. In actuality, there is nothing ‘hidden’ about food intolerance, and there is no need to resort to blood tests to find your food sensitivities.
1. Australasian Society of Clinical Immunology and Allergy. Unorthodox Techniques for the Diagnosis and Treatment of allergy, Asthma and Immune Disorders – ASCIA Position Statement [Internet]. 2007 [cited 2014 Mar 10]. Available from: http://www.allergy.org.au/health-professionals/papers/unorthodox-techniques-for-diagnosis-and-treatment (Archived by WebCite® at http://www.webcitation.org/6OjZpQGNt).
2. Stapel SO, Asero R, Ballmer-Weber BK, Knol EF, Strobel S, Vieths S, et al. Testing for IgG4 against foods is not recommended as a diagnostic tool: EAACI Task Force Report. Allergy. 2008;63(7):793–6. Available from: http://onlinelibrary.wiley.com/doi/10.1111/j.1398-9995.2008.01705.x/abstract (Archived by WebCite® at http://www.webcitation.org/6OjZbB9va).
3. Carr S, Chan E, Lavine E, Moote W. CSACI Position statement on the testing of food-specific IgG. Allergy Asthma Clin Immunol. 2012 Jul 26;8(1):12. Available from: http://www.aacijournal.com/content/8/1/12 (Archived by WebCite® at http://www.webcitation.org/6OjZmUPVA).
4. Pelsser LM, Frankena K, Toorman J, Savelkoul HF, Dubois AE, Pereira RR, et al. Effects of a restricted elimination diet on the behaviour of children with attention-deficit hyperactivity disorder (INCA study): a randomised controlled trial. The Lancet. 2011;377(9764):494–503.
5. De Magistris L, Picardi A, Siniscalco D, Riccio MP, Sapone A, Cariello R, et al. Antibodies against Food Antigens in Patients with Autistic Spectrum Disorders. BioMed Research International. 2013;2013:1–11.
6. Connor Z, Autism and autistic spectrum disorders. In: Skypala I, Venter C, editors. Food Hypersensitivity: Diagnosing and Managing Food Allergies and Intolerance. John Wiley & Sons; 2009. p. 63-68.
7. Bock SA. AAAAI support of the EAACI Position Paper on IgG4. Journal of Allergy and Clinical Immunology. 2010 Jun;125(6):1410. Available from: http://www.jacionline.org/article/S0091-6749(10)00512-9/fulltext (Archived by WebCite® at http://www.webcitation.org/6OjZkm9m9).
8. Kamdar TA, Peterson S, Lau CH, Saltoun CA, Gupta RS, Bryce PJ. Prevalence and characteristics of adult-onset food allergy. The Journal of Allergy and Clinical Immunology: In Practice. 2015 Jan;3(1):114–115.e1.
Sometimes it is easy to figure out food sensitivities – especially when they only involve one food or one kind of symptom. For example, lactose intolerance (a type of enzymatic food intolerance where people are deficient in the enzyme needed to digest milk sugar) is related only to milk and milk products, so it’s easy to notice the gastrointestinal symptoms after a nice bowl of ice cream with the kids. But other sensitivities are not so obvious.
Take pharmacological food intolerance, or just ‘food intolerance.’ This type of food sensitivity has always been hard to pin down, on both an individual level and in clinical studies. Symptoms can arise hours or even days after you eat a trigger food, and their severity depends on how much you ate, whether you ate any other trigger foods in prior days, and if you have other health conditions or environmental sensitivities. Furthermore, your symptoms may be different from those of someone else who reacts to the same foods.
On top of this, food intolerance is a reaction to chemicals that are found in a wide variety of foods. For example, if you were sensitive to histamine, you would need to watch out for fruits, meats, cheeses, chocolate, etc. If you were sensitive to artificial colors and preservatives, you would need to read every food label. This is different than food allergies, where people are oversensitive to the proteins found in specific foods. With food intolerance, your food journal wouldn’t be tracking the foods as much as the chemicals inside them. And that’s when things start to fall into place, because, as we’ll see, your symptoms aren’t always caused by the last thing that you ate.
The term ‘pharmacological food intolerance’ underscores the idea that foods, no matter how natural, can contain chemical compounds that are foreign substances in our bodies (like benzoate in fruit or artificial colors in yogurt) or excess amounts of chemicals that our bodies normally produce (like tyramine or histamine in certain cheeses). These chemicals are referred to as xenobiotics, a term which also covers substances like medications, poisons, and environmental pollutants that enter our bodies. This means that pharmacological food reactions share characteristics that are already familiar to us from our experiences with other xenobiotics. In food intolerance:
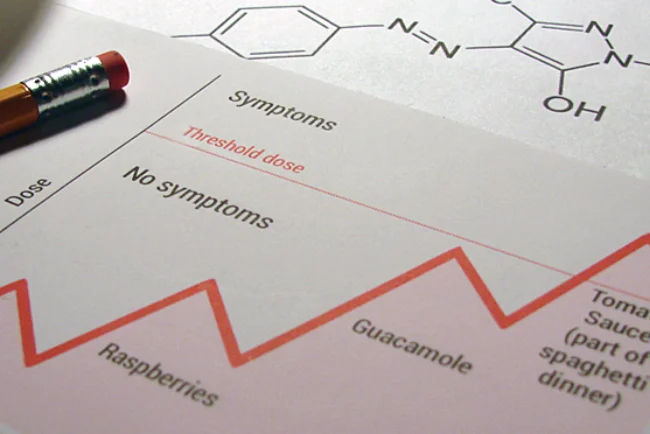
The severity of your reaction depends on the dose. Below the threshold dose, no symptoms are observed.
Doses are additive across multiple meals. What you ate throughout the day, and even the previous day, counts towards your accumulated dose. Symptoms occur when the accumulated dose exceeds the threshold dose.
Multiple food chemicals can work together to exacerbate the effects of the others.
Withdrawal symptoms can occur.
You can become temporarily tolerant of a food chemical.
The most important of these ideas is the concept of a threshold dose. If you are very sensitive to a food chemical, you have a low threshold, and a small amount is all that is needed to produce symptoms. If you have a high threshold, eating small amounts of a substance will not produce any symptoms. And it’s not necessary to consume all of your food chemical in one meal in order to exceed the threshold dose – little bits can add up over a couple of days. If you were looking to see which food caused your symptoms, you might find that it was several foods over several meals that all contained the same trigger chemical.
In general, we can say that food intolerant people have lower dose thresholds than the rest of the population since most people do not react to food. This is partly due to differences in how well the body can rid itself of chemicals and partly due to how susceptible one is to experiencing adverse reactions – this is all part of the natural variations among people. However, it turns out that your personal threshold dose can also vary over time, depending on what else you have eaten, what medications you have taken, and other health-related factors.
An example of accumulated and threshold doses
Figure: Hypothetical dosage of amines over four days. The amount of chemical trigger in your body increases as successive meals are eaten.
Consider the chart on the right that tracks meals over four days – simplified, of course, for a hypothetical person. If you experienced symptoms on Day 4, would your first inclination be to blame the spaghetti dinner and perhaps the gluten-containing pasta in particular?
Our hypothetical person is actually sensitive to salicylate and amines, and she needs a mix of both to see symptoms – it turns out that honey, raspberries, guacamole, and tomato sauce all contain at least one of these chemicals. The chemicals accumulated in her body over the course of three days until her threshold dose (which, luckily for her, is rather high) was exceeded on the fourth day.
Our person had wondered about gluten sensitivity in the past, but didn’t seem to react reliably to wheat. Now that she is mindful of her trigger chemicals and her threshold dose, she can eat some of the foods she likes without adverse effects.
How common is pharmacological food intolerance? Several million people are currently suffering from this problem in the West, and more – perhaps 5-10% – will have experienced it in their lifetime. You might see figures out there, however, that vary widely, from less than a percent to 20% and upwards, but this isn’t so surprising considering that it has also been difficult to get good prevalence estimates for food allergies (1,2). In this article we will sort through the available data and see why 5-10% is a fair estimate for the lifetime prevalence of food intolerance.
What is meant by “prevalence”?
Prevalence tells us how many people are suffering from a disorder at a single point in time, given as a percentage of the total population. Since it is impossible to ask every person whether they have a certain condition, researchers work instead with a sample of people who will represent the entire population. The size of this sample will dictate the reliability of the results. The best studies also verify a person’s response by having them go through a medical examination or some other diagnostic procedure.
What data is out there on food intolerance?
For conditions like food intolerance, where the prevalence is expected to be only a few percent (or less than a percent), the most reliable data will come from studies where the sample size is in the hundreds (or thousands). From among these studies, we only want to consider the ones that use a double blind placebo-controlled food challenge (DBPCFC) to check whether a person really suffers from food intolerance. It turns out that just a handful of investigations meet our requirements (see Table 1), and four out of five of these focus only on the effects of food additives like artificial colors and sodium benzoate.
Country
Study type
Population
Prevalence
Denmark (4) N = 4274
Additives DBPCFC
All children
1-2%
Denmark (5) N = 379
Additives OC, DBPCFC
Atopic children
2-7%
Denmark (6) N = 1094
Additives DBPCFC
22 year olds
0.5%
UK (7) N = 18,582
Additives DBPCFC
Adults
0.01%-0.23%
Germany (8) N = 4093
Foods, additives & salicylate DBPCFC
Adults
0.78-1.1%
Table 1: Selected studies on food intolerance prevalence
N is the sample size
DBPCFC is double-blind placebo-controlled food challenge, an elimination diet and food challenge where the researchers and participants are unaware of who is receiving a real food challenge or a placebo
OC is open challenge, where the challenge food is known to all involved
Overall, it appears that food additive intolerance occurs in a few percent of children and a fraction of a percent of adults; when more foods are included, as in the German study, the prevalence increases to about one percent. The studies given in Table 1 also verify what has been observed elsewhere, namely that:
Food intolerance is more common in women than in men.
Children are more likely to suffer from food additive intolerance than adults.
Atopic individuals (people with allergies and often asthma) are more likely to see adverse reactions to food, which often exacerbate flare-ups of their existing conditions.
Unfortunately, the data that we have falls short in several ways, most notably in scope. As mentioned, the studies in Table 1 focused on food additives, not naturally-occurring trigger chemicals in food. Even in terms of additives, each study differed in the number and amounts of additives that were tested, and common preservatives, such as sulphites, were absent in many cases. Madsen (3) pointed out that these studies also differed in their inclusion criteria, that is, the symptoms that people could have and still participate in a study. Furthermore, many symptoms, including migraine, gastrointestinal symptoms, and hyperactivity in children, were not considered. Thus, the reported prevalence rates are slightly lower than what should be expected for pharmacological food intolerance when it is more completely defined.
Towards a more inclusive prevalence rate
Is there any other data that we can use to improve our estimate? Numerous smaller studies have been done on food intolerance in specific groups – like sufferers of chronic skin reactions, respiratory symptoms, and gastrointestinal problems – and it is tempting to extend the numbers found there to the rest of the population. Unfortunately, we cannot rely on studies that were not originally designed to establish prevalence rates because the results may be biased. For example, specialized clinics are likely to have reputations that attract specific types of patients, and these may or may not be representative of all patients with those conditions. This is called spectrum bias, a well-known cause of variation in clinical studies.
Alternatively, we could look at prevalence estimates for sensitivities to individual food chemicals, or at the co-occurrence of food intolerance and certain illnesses, and add it all up. For example, histamine intolerance, defined as two or more non-allergic symptoms that improve through antihistamine use and a low histamine diet, is thought to have a prevalence rate of at least 1% and perhaps higher (9). In the US alone, about 12% of the population suffers from migraines, and food triggers are involved in about half the cases (10). Indirect evidence (11) suggests that irritable bowel syndrome is aggravated by foods that contain or cause the release of histamine in the body – this could affect as much as 5-10% of the population, but this has not been clinically verified. The picture is even less clear for other food triggers and conditions, and we are missing information on sensitivities to naturally-derived salicylate and benzoate, other biogenic amines, etc.
Looking at the numbers that we do have, it seems reasonable, if not conservative, that the overall prevalence of food intolerance would be at least several percent. This consistent with the lifetime prevalence estimate of 5-10% from Loblay and Swain of the RPAH Allergy Clinic in Australia (12); they based this estimate on their experience with thousands of patients, although experience does not carry the same scientific weight as epidemiological studies. Still, we can double check if these numbers make sense by considering lifetime prevalence and self-reported prevalence rates.
Lifetime prevalence
When scientists give prevalence rates, they are actually talking about point prevalence, which is how I defined prevalence at the beginning of this article: the fraction of people suffering from a disorder at a single point in time. Lifetime prevalence is the fraction of people who will suffer from a disorder at some point in their lifetime. For life-long illnesses, the point prevalence and the lifetime prevalence will be equal; for disorders that last for relatively brief periods, the lifetime prevalence can be several or even many tens of times higher than the point prevalence, depending on exactly what it is that predisposes a person to developing a disorder. We can expect that the lifetime prevalence of food intolerance will be higher than the point prevalence values we have been discussing, but we don’t know by how much.
If we have some idea of how long food intolerance lasts, we can put some limits on how many times higher lifetime prevalence could be. Food intolerance is thought of as a transient and individualized problem (13, 14). Different people will experience food intolerance for different lengths of time, and, after undergoing a period of avoiding their personal triggers, will have varying success in reintroducing these food chemicals to their diet. There are limited follow-up reports on individuals who have undergone food intolerance testing. Swain (15) found that 81% of respondents to a follow-up questionnaire still experienced a recurrence of symptoms as much as five years after having identified their trigger chemicals. We can make some assumptions and use a probability calculation to estimate that for this group, food intolerance lasts for 14 years – this means that the lifetime prevalence for adults would be about three times higher than the point prevalence. (16) This keeps us in line with our lifetime prevalence estimate of 5-10%.
Self-reported rates
Doctors and researchers often note that people perceive more adverse reactions to foods than can be verified through double-blind placebo-controlled food challenges. Self-reported prevalence rates from surveys of the general population are as much as 10 times higher than the rates determined through controlled testing – this goes for all types of food reactions, even allergies. For example, in the German study included in Table 1, which also looked at food allergy, the self-reported lifetime prevalence for all food hypersensitivities was 34.9%, while the point prevalence was found to be 3.6% based on food challenges. (8) Surveys conducted in different countries give different self-reported rates (17), which can be explained by different diets, different genetic make-ups, and cultural differences.
The discrepancy between clinical and self-reported rates causes some medical professionals to be suspicious about the existence of food intolerance. But does this discrepancy really mean that food intolerance is, for the most part, ‘all in the mind?’ Let’s consider some possible reasons for the higher self-reported rates:
Depending on the survey questions, the self-reported rates could be representing the lifetime prevalence instead of the point prevalence – we need to be careful not to compare apples and oranges.
The respondents could simply be wrong about what caused their symptoms. Most of the self-reported rates were recorded before the current media focus on food allergies and food intolerance, but, today, heightened awareness is increasing the perception that food is the source of symptoms that are otherwise unexplained.
Food aversion is a real phenomenon – you begin to associate a food with an illness and then any exposure to that food makes you feel ill – and this could be mistaken for food intolerance.
Some people may experience a food sensitivity reaction once or twice in their lives, never to be repeated. Large-scale diagnostic studies like the ones listed in Table 1 do have procedures for screening out such events (for example, see reference 7) and only inviting individuals who have a history of reproducible food-related symptoms to participate in the food challenge phase. Studies that present only self-reported rates may or may not use such procedures, so we need to look carefully at each figure to see exactly what it includes.
Another possibility is that there is something about how food intolerance is verified in clinical studies that leads to an underestimation of the true prevalence. Next we will look at the difficulties involved in diagnosing food intolerance to see if this has any effect on point prevalence.
Diagnostic challenges
While it is possible to diagnose food intolerance by elimination diets alone and by open food challenges, only the double-blind placebo-controlled food challenge (DBPCFC) is viewed by researchers as providing a definitive result. This makes it the ‘gold standard’ among test procedures, but, unlike many other gold standard tests, the accuracy of the DBPCFC is not known. (18) In other words, since the process has not been standardized, the accuracy will vary from study to study depending on how the test was conducted.
The DBPCFC was developed with food allergies in mind, where a single food is expected to produce a fairly rapid reaction. These reactions are often easy to see – an asthmatic patient experiences a decrease in breathing ability or a patient develops hives. However, even with food allergies, the results are not always clear cut. (19-21) Take chronic eczema that has not cleared before the test – how much of a change in skin irritation is needed for a positive result? How long should you wait for a response? How do you grade subjective symptoms like headache? How many times should you repeat the test if the patient responds to the placebo? Should you stop medications during the test? Etc.
The diagnosis of food intolerance shares these uncertainties and more, and it can be difficult to reproduce positive food challenge results even in people with good evidence of food intolerance. (7) Several things come into play here:
It is not uncommon for someone to need to be exposed to a combination of food chemicals before they see symptoms. For example, Di Lorenzo et al. (22) found that few patients with chronic urticaria (hives) reacted to challenges with a single food additive but that many reacted to mixtures. Something like this could result from a true sensitivity to each of the triggers (12, 15) (even ones that are not chemically related) or from the unique effects that mixtures have on the processes that rid the body of foreign chemical substances.
Food intolerance reactions are dose-dependent, so a person will only see symptoms if the accumulated amount of food chemical in their body exceeds their threshold dose. Each person has a different threshold dose and this threshold can change over time. Researchers have trouble addressing these issues in food intolerance studies. For example, high challenge doses do not necessarily guarantee more positive reactions and, in any case, might not be representative of normal consumption. Incremental challenges might seem to mimic real life, but they could also lead a person to become more tolerant of a food chemical.
Similarly, some sufferers will be more sensitive to food triggers when they are also under stress, suffering from an illness, or exposed to certain chemicals (cleaning chemicals, fragrances, etc.) in their environment. (23) These additional factors may not be present at the time of the food challenge. Hormonal changes can also play a role in food sensitivity, but I have yet to see a study account for menstrual cycle, even though more women suffer from food intolerance than men.
Patients with chronic or allergic conditions need to be experiencing symptoms at the time of the food challenge in order for any worsening effect to be observed.
Researchers could simply be testing for sensitivity to the wrong chemicals. While salicylate or histamine intolerance is most often associated with fruit, German researchers reported that patients who failed to react to those substances still reacted to tomato extract, pointing to other unknown trigger chemicals. (24, 25). In another example, Lessof (26) pointed out years ago that a reaction to pesticide residue on unwashed fruit can also mimic food intolerance.
Trying to prove an association between food intolerance and a specific condition is like a shot in the dark if the condition that you are looking at is not uniform. As an example, consider the association between attention deficit hyperactivity disorder (ADHD) in children and food additives. For decades, scientists and the public have gone back and forth over whether behavior in these children is influenced by food chemicals. In 2010, one group of researchers found that food additives affected ADHD-like symptoms in children who possessed a gene that decreased their ability to break down histamine. (27) This result has yet to be replicated, but, if verified, it would go a long way to explaining why different studies had been finding different results – only a subgroup of children with ADHD (those with a certain gene) are sensitive to food chemicals. If a study did not happen to include any of these children, then it would have found no connection between behavior and food.
Right now we do not know the extent to which these diagnostic challenges might impact clinically-determined prevalence rates for food intolerance, but we can say that there is more uncertainty in these rates than is currently understood. From the examples that I have given, you might conclude that point prevalences could only go up if researchers addressed these issues; however, it all depends on how you define food intolerance and its impact on health. Increasing the specificity of the DBPCFC would certainly benefit individuals with hard-to-diagnose food sensitivities; at the same time, large-scale prevalence studies might also find more people who experience occasional reactions that do not lead to significant impairment. In the latter case, better diagnostics would not give us any more useful information on food intolerance as a public health problem.
Since self-reported prevalence rates vary more between countries than clinically-verified rates do (see ref 16 for examples), the inflation seen in self-reported rates is probably related more to cultural effects than to limitations of the DBPCFC. Based on self-reported rates, the real lifetime prevalence of food intolerance should never be more than 20-30%, which still supports our estimate of 5-10%. If we knew more about the mechanisms behind food intolerance, we could set upper limits on the prevalence rates for sensitivities to individual trigger chemicals; however, this will not necessarily be an easy task, because for each chemical sensitivity, there are still likely to be different mechanisms at work in different people.
Conclusions
A lifetime prevalence estimate of 5-10%, as given by Loblay and Swain, is probably a good, and perhaps conservative, estimate of the true prevalence of food intolerance. Better prevalence rates will not be available until researchers standardize the double blind placebo-controlled food challenge, define food intolerance consistently in terms of trigger chemicals and recognized symptoms, and make progress uncovering the mechanisms behind food intolerance.
1. Nwaru BI, Hickstein L, Panesar SS, Muraro A, Werfel T, Cardona V, et al. The epidemiology of food allergy in Europe: a systematic review and meta-analysis. Allergy. 2014 Jan;69(1):62–75. PubMed
2. Kuznar W. Food Allergies May Not Be as Common as Reported. American Journal of Nursing. 2010 Aug;110(8):18.
3. Madsen C. Prevalence of Food Additive intolerance. Human & Experimental Toxicology. 1994 Jan 1;13(6):393–9. PubMed
4. Fuglsang G, Madsen C, Saval P, Østerballe O. Prevalence of intolerance to food additives among Danish school children. Pediatric Allergy and Immunology. 1993;4(3):123–9. PubMed
5. Fuglsang G, Madsen C, Halken S, Jørgensen M, Østergaard PA, Østerballe O. Adverse reactions to food additives in children with atopic symptoms. Allergy. 1994;49(1):31–7. PubMed
6. Osterballe M, Mortz CG, Hansen TK, Andersen KE, Bindslev-Jensen C. The Prevalence of food hypersensitivity in young adults. Pediatric Allergy and Immunology. 2009;20(7):686–92. PubMed
7. Young E, Patel S, Stoneham M, Rona R, Wilkinson JD. The prevalence of reaction to food additives in a survey population. J R Coll Physicians Lond. 1987 Oct;21(4):241–7. PubMed
8. Zuberbier T, Edenharter G, Worm M, Ehlers I, Reimann S, Hantke T, et al. Prevalence of adverse reactions to food in Germany–a population study. Allergy. 2004;59(3):338–45. PubMed
9. Maintz L, Novak N. Histamine and histamine intolerance. Am J Clin Nutr. 2007 May 1;85(5):1185–96. PubMed
10. Headache: Hope Through Research: National Institute of Neurological Disorders and Stroke (NINDS) [Internet]. [cited 2013 Dec 1]. Available from: http://www.ninds.nih.gov/disorders/headache/detail_headache.htm (Archived by WebCite® at http://www.webcitation.org/6Ojafedcl).
11. Smolinska S, Jutel M, Crameri R, O’Mahony L. Histamine and gut mucosal immune regulation. Allergy. 2013 Nov 29; PubMed
13. Pollock I, Warner JO. A follow-up study of childhood food additive intolerance. J R Coll Physicians Lond. 1987 Oct;21(4):248–50. PubMed
14. Hayder H, Mueller U, Bartholomaeus A. Review of Intolerance Reactions to Food and Food Additives. International Food Risk Analysis Journal. 2011;1.
15. Swain A. The role of natural salicylates in food intolerance [Internet] [PhD Dissertation]. University of Sydney; 1988.
16. Assumptions: The disappearance of symptoms follows a fixed probability and can be modelled by an exponential distribution; 81% still experience symptoms after 3 years. The rate of decline would be 0.07 events/year, which would lead to an expectation of 1/0.07 ≈ 14 years/event. For adults, assume a lifetime period of 40 years: 40/14 ≈ 3.
17. Skypala I. Other Causes of Food Hypersensitivity. In: Skypala I, Venter C, editors. Food Hypersensitivity: Diagnosing and Managing Food Allergies and Intolerance. John Wiley & Sons; 2009. p. 210–42.
18. Gellerstedt M, Bengtsson U, Niggemann B. Methodological issues in the diagnostic work-up of food allergy: a real challenge. Journal of Investigational Allergology and Clinical Immunology. 2007;17(6):350. PubMed
19. Niggemann B, Beyer K. Pitfalls in double-blind, placebo-controlled oral food challenges. Allergy. 2007 Jun 15;62(7):729–32. PubMed
20. Bindslev-Jensen C. Standardization of double-blind, placebo-controlled food challenges. Allergy. 2001;56(s67):75–7. PubMed
21. Niggemann B. When is an oral food challenge positive? Allergy. 2010 Jan;65(1):2–6. PubMed
22. Di Lorenzo G, Pacor ML, Mansueto P, Martinelli N, Esposito-Pellitteri M, Lo Bianco C, et al. Food-additive-induced urticaria: a survey of 838 patients with recurrent chronic idiopathic urticaria. Int Arch Allergy Immunol. 2005 Nov;138(3):235–42. PubMed
23. Allen DH, Van Nunen S, Loblay R, Clarke L, Swain A. Adverse reactions to foods. Med J Aust. 1984 Sep 1;141(5 Suppl):S37–42. PubMed
24. Henz BM, Zuberbier T. Most chronic urticaria is food-dependent, and not idiopathic. Exp Dermatol. 1998 Aug;7(4):139–42. PubMed
25. Zuberbier T, Pfrommer C, Specht K, Vieths S, Bastl-Borrmann R, Worm M, et al. Aromatic components of food as novel eliciting factors of pseudoallergic reactions in chronic urticaria. J Allergy Clin Immunol. 2002 Feb;109(2):343–8. PubMed
27. Stevenson J, Sonuga-Barke E, McCann D, Grimshaw K, Parker KM, Rose-Zerilli MJ, et al. The role of histamine degradation gene polymorphisms in moderating the effects of food additives on children’s ADHD symptoms. Am J Psychiatry. 2010 Sep;167(9):1108–15. PubMed
In this day and age, it’s hard to imagine medical tests that don’t draw blood or that don’t involve expensive, room-filling equipment; however, for food intolerance and some immune-mediated reactions, the tried and true diagnostic requires only a pencil, paper, and food. Doctors, dietitians, and medical researchers rely on elimination diets and food challenges to identify food sensitivities, which can be used regardless of the underlying mechanism – this is important because right now we have only rough ideas of how these some of these reactions might work.
Diet investigations are deceptively simple – start from scratch and add only one potential trigger at a time until the culprit is found – but they also require a detailed knowledge of food chemicals. For this and for safety reasons – after all, you need to rule out if you actually have an allergy or another condition – you should always undergo a diet investigation with the help of a doctor or a registered dietitian. To help you prepare, let’s look at the three phases of the process: the elimination diet, the food challenges, and the modified diet. Before you start, your dietitian may also ask you to briefly keep a food and symptom journal to provide a baseline on the severity and frequency of your symptoms.
Caution: The information here is provided to give you an idea of the diet investigation process; it is not a set of instructions to carry out the procedure yourself. Always check with a doctor or a registered dietitian before modifying your diet. The elimination diet/food challenge process is not appropriate for pregnant women. People with asthma or laryngeal edema (swelling in the throat/upper airways) should only undergo food challenges in a clinic where resuscitation facilities are available. People with Crohn’s disease should not try an elimination diet without medical supervision.
Phase 1: Elimination diet
The elimination diet consists of only a few foods that are unlikely to cause symptoms in most people; depending on your history, it might be less restrictive. You must adhere to the diet even if you think that you know which food chemical makes you ill because you might be sensitive to more than one chemical. In most people, symptoms improve after two to four weeks on the elimination diet. You may experience a withdrawal reaction (a flare-up of symptoms) after the first or second week.
The elimination diet is necessary for several reasons. First, it indicates whether you are on the right track: if there is no change in symptoms after four weeks of strict adherence to the diet, then food intolerance is unlikely. Second, it removes the variability (the ‘noise’) in your symptoms so that changes can be detected during the food challenge phase. Finally, it lowers the amount of trigger chemical that you need to eat in order to see symptoms.
Phase 2: Food challenges
The food challenges determine which food chemicals are triggering symptoms. After at least two weeks on the elimination diet, specific foods are reintroduced into your diet one at a time – these are the ‘challenges.’ If a reaction occurs after a challenge, then you must wait until the symptoms subside, plus a few days, before moving on to the next food. Such challenges are referred to as ‘open’ challenges because you are aware of what you are eating. In research studies, participants are given food chemicals in capsules so they do not know which chemical is being tested or whether they are getting a placebo – these ‘blind’ challenges provide the most reliable diagnosis.
Wheat and milk are often tested first because reactions to these foods are just as common as pharmacological food intolerance reactions; then salicylate, benzoate, amines, MSG, artificial colors, etc. are tested on the advice of your dietitian. Ideally, challenge foods would only contain one trigger chemical, but this is not always possible. When challenge foods contain more than one trigger, the ordering of the challenges is important to systematically rule out all possibilities.
Your dietitian will design a modified diet for you based on your challenge results. You will be reevaluated in 1 or 2 months to see how well the restricted diet is working and to decide whether it is safe to liberalize what you eat. In this part of the process, you will be checking to see whether you have a high or low dose threshold for symptoms; you may also be able to gradually increase the amount of triggers that you eat, but, for your safety, you should always work on this with a dietitian or doctor. Since threshold doses can decrease after avoiding a food chemical, sensitive people could experience dangerous reactions when reintroducing foods to their diet, even in amounts that previously did not cause symptoms.
More information
Consult these books if you are interested in learning more about diet investigations:
RPAH Elimination Diet Handbook with food and shopping guide by Swain, Soutter and Loblay of the Royal Prince Alfred Hospital Allergy Unit
Brostoff J, Gamlin L. Food Allergies and Food Intolerance: The Complete Guide to Their Identification and Treatment. Inner Traditions/Bear; 2000. 486 p.
Clarke L, McQueen J, Samild A, Swain A. The dietary management of food allergy and food intolerance in children and adults. Australian Journal of Nutrition and Dietetics. 1996;53(3):89–98.
Food intolerance is a broad label that describes adverse reactions to food that do not involve the immune system. This site uses the term food intolerance as it has been defined by the Allergy Unit at the Royal Prince Alfred Hospital in Australia, which corresponds to what some call pharmacological food intolerance.
What is food intolerance?
Food intolerance occurs when chemicals in food produce side effects, similar to the way that drugs produce side effects. Some people are more sensitive to these effects than others.
Food intolerance is not an allergy. A food allergy is an oversensitivity to a protein in a specific food, while food intolerance is a sensitivity to chemicals found in a wide variety of foods.
Organic, fresh, or processed foods can all cause adverse reactions – not all trigger chemicals are man-made.
Symptoms can be physical or behavioral, especially in children. Some people suffer from more than one symptom, and symptoms can change over time.
Food intolerance may affect up to 10% of the population when all food chemicals are considered, which is at least 2 times the prevalence of food allergy. Still, this means that food intolerance is relatively rare: for each food chemical, perhaps 99% of the population will experience no adverse effects.
Food intolerance is more common in adults than in children. Lifestyle factors may play a part in this. In comparison, more children suffer from food allergies than adults.
Children with food intolerance are more likely to be sensitive to food additives (artificial colors, flavors, and preservatives) than adults.
Food intolerance seems to run in families, although each family member may be sensitive to a different food chemical. More women experience food intolerance than men.
Food intolerant people are also likely to suffer from allergies. Food intolerance can make existing flare-ups of eczema and asthma worse, but cannot bring about these conditions on its own.
When do people experience food intolerance symptoms?
Symptoms can take hours to days to appear.
The severity of symptoms depends on how much of a food chemical was eaten, even over the course of several days.
Since symptoms are dose-dependent, they may seem unpredictable – sometimes they happen, sometimes they don’t. But if you think of food in terms of its chemical constituents, it all starts to make sense.
Some people are sensitive to more than one chemical and need to eat them in combination in order to see symptoms. Others only experience symptoms when they are under stress, sick, or have been exposed to chemicals in their environment.
Food intolerance should be considered only after your doctor has ruled out food allergies and other conditions and has given you the go ahead.
An elimination diet followed by food challenges is the only way to diagnose food intolerance.
Foods can contain more than one trigger chemical, making the order of the food challenges very important for ruling out all possible triggers. A registered dietitian can help.
Imagine that you are in a Chinese restaurant with your family. You’ll probably get a migraine later tonight (maybe from the amines in the soy sauce), but you’ve been craving Chinese food all week and you haven’t made the connection yet. Your daughter is drinking cup after cup of jasmine tea with her five spice stir fry, and this, combined with the other things she ate during the day, will give her hives again this evening. Your son asks you to read the fortune in his fortune cookie – “Knowledge is power,” it says, but it doesn’t warn you about the tartrazine in the cookie. He’ll be cranky tonight and distracted tomorrow morning. This is what you might experience if you suffer from food intolerance.
Lesson 1: What is food intolerance?
Food intolerance, as defined by the Allergy Unit at the Royal Prince Alfred Hospital in Australia, is a sensitivity to chemicals found in a wide variety of foods. It is also known as pharmacological food intolerance, a type of non-allergic food hypersensitivity. Food intolerance does not involve the immune system.
Is food intolerance real?
Yes. The existence of pharmacological food intolerance has been established by double blind placebo-controlled food challenges. The bulk of the research on food intolerance has been conducted in Australia, the UK, and Germany, and there is an increased awareness of food intolerance in these countries.
That said, two points should be kept in mind. First, even though food intolerance is real, it is relatively rare. These reactions are aptly categorized as ‘hypersensitivity’ reactions, meaning that most people – perhaps 99% depending on the substance – will not experience any problems from food chemicals at normal amounts. Second, not all evidence carries equal weight when it comes to the different trigger chemicals, and many questions still need to be answered.
The term ‘pharmacological’ is related of the nature of the substances that elicit food intolerance reactions. In addition to nutrients, foods contain chemicals that are foreign to our bodies (like benzoate in fruit or artificial colors in yogurt) or excess amounts of chemicals that our bodies normally produce (like tyramine or histamine in certain cheeses). This is obvious in the case of processed foods, but it is true for fresh or organic foods as well. The foreign or excess chemicals are processed in the body along the same lines as drugs, and in food intolerant people, they also produce drug-like effects. But why would such chemicals be present naturally in food? Because they are important to plants or because they are part of the normal ripening and aging processes.
Food intolerance is different in each person. Some people will be sensitive to certain trigger chemicals for their entire life, and these people will need to avoid foods that contain these chemicals in order to remain symptom-free. Others will only need to avoid their culprit foods for a time until they can resume eating them – perhaps in limited quantities – without seeing symptoms. Still others might only see problems when they eat large amounts of their offending foods or eat certain combinations of foods. But for everyone, the key to living life to the fullest is an accurate determination of which food chemicals are causing the problem. A registered dietitian or doctor can help you find your triggers through an elimination diet and food challenges.
Lesson 2: Food triggers linked to food intolerance
Table 1 contains the most commonly discussed food triggers linked to food intolerance. More than one trigger can be present in a given food, making it difficult to determine which foods contributed to your symptoms. Please be aware, though, that not all of the chemicals listed below are implicated in food intolerance by the same degree of evidence — for all the details, I recommend this open-access review:
Food intolerance symptoms can arise hours or even days after eating a trigger food, and their severity depends on how much you ate, what you ate during the previous few days, and whether you have other health conditions. On top of this, symptoms can be aggravated by illness, environmental chemicals (like fragrances), medications, hormonal changes, or stress. The most common symptoms of food intolerance are given below.
System
Symptom
Skin
Hives (urticaria), swelling (angioedema), itching, aggravation of eczema
Migraine, vertigo, fatigue, muscle pain (myalgia), growing pains, behavioral changes in children
Generalized
Non-immune anaphylaxis
Table 2: Possible symptoms of pharmacological food intolerance
Lesson 4: Food intolerance as a food hypersensitivity
Adverse reactions like food intolerance and food allergy are classified as hypersensitivity reactions, where the concept of hypersensitivity has real meaning. Food hypersensitivities are reproducible reactions brought about by quantities of foods that most people can tolerate. In other words, to classify an adverse reaction as a food hypersensitivity, you must first think about the effect that a normal amount of that food would have on the average person.
Food hypersensitivities are divided into two main groups: those that are caused by the immune system (immune-mediated hypersensitivities) and those that aren’t (non-immune mediated hypersensitivities). If we consider food allergy – the poster child for immune-mediated food hypersensitivities – it is easy to see why hypersensitivity is an appropriate description. Allergies occur when the immune system overreacts to harmless proteins in foods, like milk, eggs, wheat, and soy, that lie at the heart of the Western diet. Only about 5% of the overall population is suffering from some type of food allergy, and the amount of food needed to trigger an allergic reaction can be much less than a typical portion.
There are more immune-mediated food hypersensitivities than just food allergies. These reactions involve other aspects of the immune system and may take a longer time to develop than a classic allergic reaction. Here I’m talking about problems like cow’s milk protein intolerance, soy protein intolerance and food protein induced entercolitis in children, celiac disease, and eosinophilic esophagitis — in some cases, asthma and eczema are also related to food. Notice that these conditions are occasionally lumped under food intolerance (and ‘intolerance’ even appears in a few of the labels), but strictly speaking, these are immune reactions.
The term food intolerance is used as the common name for non-immune mediated food hypersensitivities. The best-known type of food intolerance is lactose intolerance, the gastrointestinal discomfort that results from undigested lactose (milk sugar) in the colon. Roughly 75% of the world’s adults — 25% in the US and even fewer in northern Europe — do not produce enough lactase to digest all of the lactose they consume, but not all of these people will experience symptoms and, thus, lactose intolerance. In lactose intolerance, symptoms depend on a person’s gut bacteria and eating habits.
Pharmacological food intolerance, the focus of this primer, is also a non-immune mediated food hypersensitivity. For example, consider a person who has worked with their doctor to determine that their headaches and diarrhea are symptoms of histamine intolerance. In histamine intolerance, a person’s ability to break down histamine is impaired, so foods that are rich in histamine or that cause histamine to be released in the body can lead to symptoms. Histamine intolerance is a food hypersensitivity, because most people can tolerate normal quantities of histamine-rich or histamine-releasing foods.
That said, how do we gauge what “most people” can tolerate? As with food allergy and other immune-mediated food hypersensitivities, the non-immune hypersensitivities generally affect less than 10 or even less than 5% of the population. For example, less than 1% of adults are sensitive to food additives, at least 1% have histamine sensitivity, and around 6% suffer from food-induced migraines. This means that for any food hypersensitivity, perhaps 99% of people will experience no adverse reactions to those foods or food chemicals.
Allen DH, Van Nunen S, Loblay R, Clarke L, Swain A. Adverse reactions to foods. Med J Aust. 1984 Sep 1;141(5 Suppl):S37–42. PubMed
Brown-Esters O, Mc Namara P, Savaiano D. Dietary and biological factors influencing lactose intolerance. International Dairy Journal. 2012 Feb;22(2):98–103.
Committee on toxicity of chemicals in food, consumer products and the environment. Adverse reactions to foods and food ingredients. London: Food Standards Agency; 2000.
Hodge L, Swain A, Faulkner-Hogg K. Food allergy and intolerance. Aust Fam Physician. 2009 Sep;38(9):705–7. PubMed
Johansson SGO, Hourihane J, Bousquet J, Bruijnzeel-Koomen C, Dreborg S, Haahtela T, et al. A revised nomenclature for allergy: an EAACI position statement from the EAACI nomenclature task force. Allergy. 2001;56(9):813–24. PubMed
Joneja JMV. The Health Professional’s Guide to Food Allergies and Intolerances. Academy of Nutrition & Dietetics; 2012. 477 p.